Have you ever discovered how to do something - and wished you'd known about it before? We hope so- that's why psychologists say learning is an even more important motivation than sex to joyful adult people. Consider this recommendation for spending 3 minutes of your time
3 MINUTE EXERCISE
If many people are meeting each other for the first time- including a new class at school - we recommend spending the first 3 minutes: ask people to stand up in groups of three- each person spends 60 seconds on the greatest life changing moment in her life to date and what she started doing differently because of it.
Q&A- 1) why's this smart way spending 3 minutes introducing people? 2) how to action debrief everyone after first 3 minutes? 3) what other tools exist for innovating simultaneous communications-doing among masses of people? 4) Does our species' future generation depend on experiencing such culturally simple and trustworthy ways to spend time communicating?
Let's discuss q4 first:
You may have heard that in 2015 all our national leaders at the United Nations listed 17 SDG: Sustainability Development Goals- challenges to organise our lives at work and play around if we want out children to have a future.
(By the way most peoples' minds cant organise round doing 17 tasks at the same time - so if there was one goal that connected all the others of being human: -
true or false- the world you and I and every human being can most celebrate is one where each next girl or boy born has a good chance at living a happy free and productive life. (This is sometimes called goal 1 end poverty -it is linked to other basic goals 2 end people dying of hunger, 3 end people dying of any disease parents/communities could prevent or cure if education networks has shared information openly ...) See future shocking footnote for more
If every time you met a large group of strangers, the first 3 minutes was spent on the above exercise then you would get an idea of the community you were about to spend more time with as well as some particular people you most wanted to "friend" ie network with further, or the opposite! Of course there are times - eg when you are a child - that you may not be free to exercise this freedom of speech/action. Elders (eg parents) may have chosen this for you. Assuming you are connected to elders who love you, then their values should be your safety, physical and mental health and whats smart for your being to find your place in the world. Places and nations depend on getting this right as the sustainability goals themselves offer living testimony to. Healthy youthful societies generate economic growth not vice versa. If professions including judges do not agree this as their hippocratic hypothesis for being , then darkness descends, light may not return.
Its a measure that something has gone wrong with places; media and measurements if young people are voicing concerns - eg greta on climate - and old people are not showing they are listening by changing how everyone spends their time - especially teachers and students and your home community spends your time tomorrow and tomorrow as the Bard memorilaised
We are not saying all of this is easy. Nor are other things we spend the first 11,14 or 18 years of life on depending how long your place designs schools around. But tools like the 3 minute exercise help experiencing what matters to people through life. How does one search for networks who link into methods like these. We recommend starting with (alumni of ) Harrison Owen. If you have a different favorite starTing point the world Of teachers and students could celebrate knowing of - please share - chris.macrae@yahoo.co.uk
Shocking Footnote
Something accidentally weird happened when man started to develop machine engineering in 1760 - Glasgow University James Watt. At that time and for the next 100 years England representing less than half a per cent of peoples on earth was the most superpowerful hub of trade and knowhow in the world. Their higher education colleges, oxbridge, were extremely influential. They determined what children who spoke the english language spent their time being examined on. For some reason -SEE THIS REFERENCE from diary of World Record Job Creator Adam Smith - the empire's higher education system did not make goal 1 ending poverty its overarching "values" purpose. In fact, we are not sure that a university system began to be designed around Goal 1's purpose until 2001 when Fazle Abed decided that 30 years of empowering the worlds poorest women to end poverty was a worthy alumni network for a humanly innovative 21st c university
Henry Dunant
Biographical
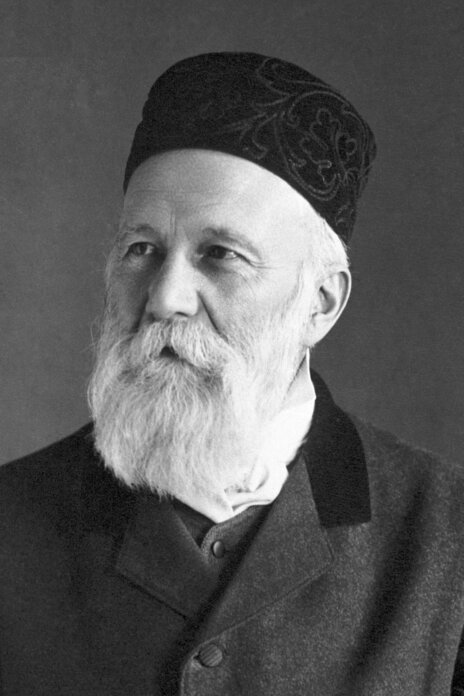
 Jean Henry Dunant‘s life (May 8, 1828-October 30, 1910) is a study in contrasts. He was born into a wealthy home but died in a hospice; in middle age he juxtaposed great fame with total obscurity, and success in business with bankruptcy; in old age he was virtually exiled from the Genevan society of which he had once been an ornament and died in a lonely room, leaving a bitter testament. His passionate humanitarianism was the one constant in his life, and the Red Cross his living monument.
Jean Henry Dunant‘s life (May 8, 1828-October 30, 1910) is a study in contrasts. He was born into a wealthy home but died in a hospice; in middle age he juxtaposed great fame with total obscurity, and success in business with bankruptcy; in old age he was virtually exiled from the Genevan society of which he had once been an ornament and died in a lonely room, leaving a bitter testament. His passionate humanitarianism was the one constant in his life, and the Red Cross his living monument.
The Geneva household into which Henry Dunant was born was religious, humanitarian, and civic-minded. In the first part of his life Dunant engaged quite seriously in religious activities and for a while in full-time work as a representative of the Young Men’s Christian Association, traveling in France, Belgium, and Holland.
When he was twenty-six, Dunant entered the business world as a representative of the Compagnie genevoise des Colonies de Sétif in North Africa and Sicily. In 1858 he published his first book, Notice sur la Régence de Tunis [An Account of the Regency in Tunis], made up for the most part of travel observations but containing a remarkable chapter, a long one, which he published separately in 1863, entitled L’Esclavage chez les musulmans et aux États-Unis d’Amérique [Slavery among the Mohammedans and in the United States of America].
Having served his commercial apprenticeship, Dunant devised a daring financial scheme, making himself president of the Financial and Industrial Company of Mons-Gémila Mills in Algeria (eventually capitalized at 100,000,000 francs) to exploit a large tract of land. Needing water rights, he resolved to take his plea directly to Emperor Napoleon III. Undeterred by the fact that Napoleon was in the field directing the French armies who, with the Italians, were striving to drive the Austrians out of Italy, Dunant made his way to Napoleon’s headquarters near the northern Italian town of Solferino. He arrived there in time to witness, and to participate in the aftermath of, one of the bloodiest battles of the nineteenth century. His awareness and conscience honed, he published in 1862 a small book Un Souvenir de Solférino [A Memory of Solferino], destined to make him famous.
A Memory has three themes. The first is that of the battle itself. The second depicts the battlefield after the fighting – its «chaotic disorder, despair unspeakable, and misery of every kind» – and tells the main story of the effort to care for the wounded in the small town of Castiglione. The third theme is a plan. The nations of the world should form relief societies to provide care for the wartime wounded; each society should be sponsored by a governing board composed of the nation’s leading figures, should appeal to everyone to volunteer, should train these volunteers to aid the wounded on the battlefield and to care for them later until they recovered. On February 7, 1863, the Société genevoise d’utilité publique [Geneva Society for Public Welfare] appointed a committee of five, including Dunant, to examine the possibility of putting this plan into action. With its call for an international conference, this committee, in effect, founded the Red Cross. Dunant, pouring his money and time into the cause, traveled over most of Europe obtaining promises from governments to send representatives. The conference, held from October 26 to 29, with thirty-nine delegates from sixteen nations attending, approved some sweeping resolutions and laid the groundwork for a gathering of plenipotentiaries. On August 22, 1864, twelve nations signed an international treaty, commonly known as the Geneva Convention, agreeing to guarantee neutrality to sanitary personnel, to expedite supplies for their use, and to adopt a special identifying emblem – in virtually all instances a red cross on a field of white1.
Dunant had transformed a personal idea into an international treaty. But his work was not finished. He approved the efforts to extend the scope of the Red Cross to cover naval personnel in wartime, and in peacetime to alleviate the hardships caused by natural catastrophes. In 1866 he wrote a brochure called the Universal and International Society for the Revival of the Orient, setting forth a plan to create a neutral colony in Palestine. In 1867 he produced a plan for a publishing venture called an «International and Universal Library» to be composed of the great masterpieces of all time. In 1872 he convened a conference to establish the «Alliance universelle de l’ordre et de la civilisation» which was to consider the need for an international convention on the handling of prisoners of war and for the settling of international disputes by courts of arbitration rather than by war.
The eight years from 1867 to 1875 proved to be a sharp contrast to those of 1859-1867. In 1867 Dunant was bankrupt. The water rights had not been granted, the company had been mismanaged in North Africa, and Dunant himself had been concentrating his attention on humanitarian pursuits, not on business ventures. After the disaster, which involved many of his Geneva friends, Dunant was no longer welcome in Genevan society. Within a few years he was literally living at the level of the beggar. There were times, he says2, when he dined on a crust of bread, blackened his coat with ink, whitened his collar with chalk, slept out of doors.
For the next twenty years, from 1875 to 1895, Dunant disappeared into solitude. After brief stays in various places, he settled down in Heiden, a small Swiss village. Here a village teacher named Wilhelm Sonderegger found him in 1890 and informed the world that Dunant was alive, but the world took little note. Because he was ill, Dunant was moved in 1892 to the hospice at Heiden. And here, in Room 12, he spent the remaining eighteen years of his life. Not, however, as an unknown. After 1895 when he was once more rediscovered, the world heaped prizes and awards upon him.
Despite the prizes and the honors, Dunant did not move from Room 12. Upon his death, there was no funeral ceremony, no mourners, no cortege. In accordance with his wishes he was carried to his grave «like a dog»3.
Dunant had not spent any of the prize monies he had received. He bequeathed some legacies to those who had cared for him in the village hospital, endowed a «free bed» that was to be available to the sick among the poorest people in the village, and left the remainder to philanthropic enterprises in Norway and Switzerland.
| Selected Bibliography |
| Les Débuts de la Croix-Rouge en France. Paris, Librairie Fischbacher, 1918. |
| Dunant, J. Henri. His manuscripts are held by the Bibliothèque publique et universitaire de Genève. |
| Dunant, J. Henry, A Memory of Solferino. London, Cassell, 1947. A translation from the French of the first edition of Un Souvenir de Solférino, published in 1862. The author published the original as «J. Henry Dunant», although he is usually referred to as «Henri Dunant». |
| Gagnebin, Bernard, «Le Rôle d’Henry Dunant pendant la guerre de 1870 et le siège de Paris», bound separately but originally published in Revue internationale de la Croix-Rouge (avril, 1953). |
| Gigon, Fernand, The Epic of the Red Cross or the Knight Errant of Charity, translated from the French by Gerald Griffin. London, Jarrolds, 1946. |
| Gumpert, Martin, Dunant: The Story of the Red Cross. New York, Oxford University Press, 1938. |
| Hart, Ellen, Man Born to Live: Life and Work of Henry Dunant, Founder of the Red Cross. London, Gollancz, 1953. |
| Hendtlass, Willy, «Henry Dunant: Leben und Werk», in Solferino, pp. 37-84. Essen Cityban, Schiller, 1959. |
| Hommage à Henry Dunant. Genève, 1963. |
| Huber, Max, «Henry Dunant», in Revue internationale de la Croix-Rouge, 484 (avril, 1959) 167-173. A translation of a brief sketch originally published in German in 1928. |
1. The emblem in Muslim countries is the red crescent and in Iran is the red lion and sun. (For a brief history of the Red Cross see history of the Red Cross.)
2. «Extraits des mémoires» in Les Débuts de la Croix-Rouge en France, p. 72.
3. Taken from a letter written by Dunant and published by René Sonderegger; quoted by Gigon in The Epic of the Red Cross, p. 147.
This autobiography/biography was written at the time of the award and first published in the book series Les Prix Nobel. It was later edited and republished in Nobel Lectures. To cite this document, always state the source as shown above.